Facilitators
Dr Seth Asafu — professional psychologist and lecturer at the University of Ghana — is leading the sessions. He brings extensive experience in psychosocial support across diverse contexts. Mr Caleb, also from the University of Ghana, Accra, is co-facilitating and supporting practical exercises and group reflections.
Day One Highlights
The first day focused on understanding trauma and how it affects both survivors and caregivers. The team reflected on common traumatic experiences encountered in social work and discussed how caregivers can become affected when they empathize deeply with clients’ stories. Trauma was defined as a response to an overwhelming negative experience and described in three forms: acute, chronic, and complex, depending on frequency and duration of harm.
Facilitators emphasized that children often experience trauma through physical abuse, domestic violence, and sexual abuse. When children disclose these experiences, staff may mirror those emotions and feel secondary trauma. The team practiced grounding techniques, including the 5-4-3-2-1 sensory method to help stabilize individuals in distress.
Responses to Danger and Trauma Assessment
In the second session, the team explored how people respond to danger using the fight, flight, fawn, or freeze framework. Facilitators stressed the importance of trauma-informed assessment for social service providers. Key reasons for trauma assessment were outlined:
- Provide appropriate interventions and support
- Prevent misdiagnosis such as mistaking trauma for bad behaviour
- Determine severity, risk, and resilience factors
Key principles of trauma-informed practice were reviewed:
- Safety first both emotional and physical
- Do no harm avoid re-traumatization
- Cultural sensitivity and confidentiality
- Build trust before deep exploration
 During assessments, staff were encouraged to focus on trauma exposure, symptoms and responses, functioning, risk, and protective factors.
During assessments, staff were encouraged to focus on trauma exposure, symptoms and responses, functioning, risk, and protective factors.
Approaches and Tools
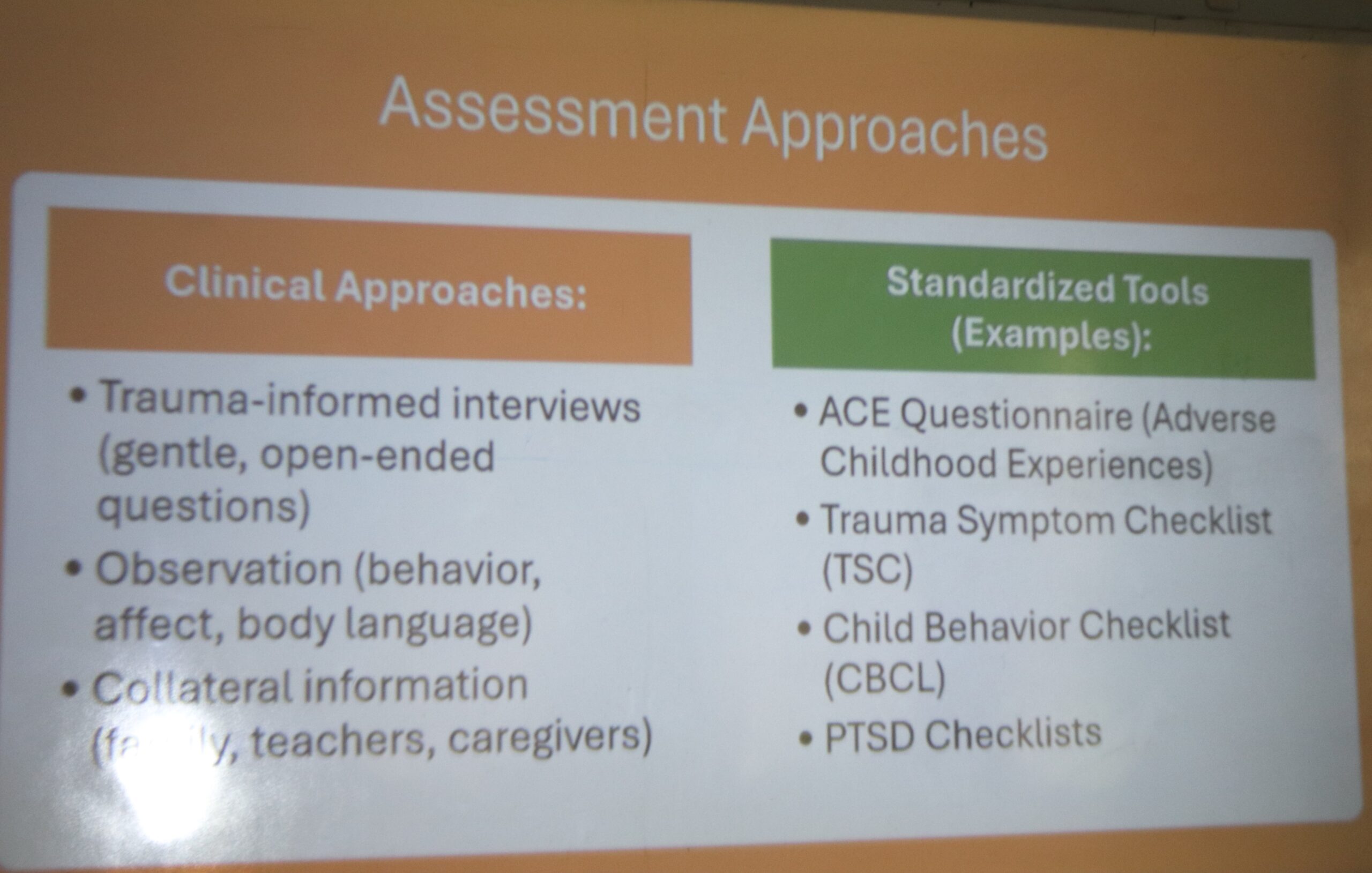
The training covered two broad approaches: clinical methods and standardized tools. Clinical methods include trauma-informed interviews, observations, and gathering collateral information. Standardized tools discussed were Adverse Childhood Experiences (ACE), Trauma Symptom Checklist (TSC), Childhood Behavioural Checklist (CBCL), and Post-Traumatic Stress Disorder screening.
The facilitators emphasized combining clinical judgment with standardized measures to form a complete picture of a child’s needs.
Case Scenarios and Closing
Day one concluded with two case scenarios to apply learning. The first involved a woman whose past relationship abuse has left lasting effects on her relationships. The second focused on a young girl with very low self-esteem and fear after persistent verbal abuse and community stigma following her mother’s death. These scenarios helped the team practice assessment, empathic response, and appropriate intervention planning.
The psychosocial therapy sessions continue tomorrow. The team looks forward to leaving the retreat more empowered, resilient, and better equipped to serve children and families with compassion and professionalism.